Using Electrophysiology to Study Cardiac Arrhythmias: Tools and Protocols

Written By: Craig Bradley
Oct 15, 2025
GEMINI (2025) The precise investigation of electrical impulse formation and conduction across myocardial tissues is critical for understanding the pathology of cardiac arrhythmias. Electrophysiology serves as the indispensable discipline for characterizing the molecular and cellular mechanisms underpinning these conditions, which remain a significant global health burden. The application of advanced recording techniques allows laboratory professionals to isolate and measure specific ion channel currents, action potentials, and tissue-level propagation patterns, bridging the gap between molecular defects and observable clinical phenotypes associated with cardiac arrhythmias. The following outlines the core instrumentation and methodological protocols that facilitate rigorous investigation into the etiology and progression of cardiac arrhythmias. Understanding the functional consequences of genetic variants in ion channel genes (channelopathies) is fundamental to the study of inherited cardiac arrhythmias. Traditional manual patch-clamp electrophysiology, while highly precise, presents limitations in throughput, making it impractical for large-scale compound screening or rapid phenotypic analysis of patient-derived induced pluripotent stem cell-derived cardiomyocytes (iPSC-CMs). High-throughput automated patch-clamp (HT-APC) systems have transformed this area of research. These platforms utilize disposable microfluidic chips to perform parallel recordings, significantly increasing the volume of data that can be acquired for defining the kinetic properties of cardiac ion channels. The transition from manual to automated systems is particularly critical for characterizing currents directly implicated in cardiac arrhythmias, such as: The HT-APC workflow includes automated cell dispensing, seal formation (Gigaohm seals), and rapid solution exchange, allowing for robust concentration-response curve generation and voltage-dependent inactivation studies. Implementing strict quality control metrics, such as monitoring seal resistance and series resistance drift, is essential to ensure the electrophysiological integrity of the recorded currents and to guarantee the reliability of data used to predict arrhythmogenic risk. The ability to quickly and accurately profile ion channel activity is key to identifying potential pharmacological agents that can correct or stabilize the electrical function impaired by cardiac arrhythmias. While patch-clamp focuses on single-cell events, optical mapping provides a holistic view of electrical propagation across intact tissue or whole-heart preparations. This technique employs voltage-sensitive dyes (VSDs) and/or calcium-sensitive dyes (CSDs) combined with high-speed, high-resolution cameras to capture spatiotemporal dynamics—an indispensable approach for visualizing the complex re-entrant circuits characteristic of severe cardiac arrhythmias. Optical mapping experiments are typically conducted on Langendorff-perfused whole hearts, ventricular slices, or monolayer cultures of iPSC-CMs. The protocol requires careful consideration of several variables to achieve accurate readings: Minimizing Motion Artifacts: The heart’s natural mechanical contraction must be mitigated to prevent movement from interfering with the optical signal. This is achieved through mechanical uncouplers, such as blebbistatin, which inhibit myosin II activity without significantly altering the VSD signal that measures transmembrane potential. Dye Selection: Voltage dyes (e.g., Di-4-ANEPPS) must be photo-stable and efficiently incorporated into the membrane. The excitation light source (LED or laser) must match the dye's spectrum while minimizing phototoxicity. Signal Processing: Raw optical signals require filtering to remove noise and normalization to account for non-uniform dye loading. The output is a sequence of activation maps that visualize impulse conduction velocity, restitution properties, and the precise trajectory of electrical waves. This methodology is crucial for studying the mechanisms underlying ventricular fibrillation (VF) and atrial fibrillation (AF), which are the most common and life-threatening cardiac arrhythmias. Optical mapping facilitates the identification of critical electrophysiological events that initiate and sustain re-entry: Parameter Analyzed Importance in Cardiac Arrhythmias Research Conduction Velocity Quantifies tissue excitability; reduction indicates a substrate for re-entry. Action Potential Duration (APD) Measures repolarization; excessive dispersion of APD is arrhythmogenic. Wavelength ( Determines the size of a re-entrant circuit ( Phase Singularity Analysis Identifies the core (or pivot point) of spiral waves and rotors that drive fibrillatory cardiac arrhythmias. Translational research often necessitates the use of in vivo animal models (typically rodent or large animal) to study the integrated effects of cardiac arrhythmias on the whole organism. Standardized protocols utilizing programmed electrical stimulation (PES) are employed to induce and characterize arrhythmogenic susceptibility. These protocols closely parallel those used in clinical settings and require precise, fractionated current delivery via pacing catheters. The S1-S2 protocol, a cornerstone of arrhythmogenesis assessment, involves delivering a train of eight fixed-interval stimuli (S1) followed by a premature stimulus (S2) at progressively shorter coupling intervals. The primary goal is to determine the ventricular effective refractory period (VERP) and the vulnerability threshold for inducing sustained or non-sustained ventricular cardiac arrhythmias, such as ventricular tachycardia (VT). More sophisticated protocols involve S1-S2-S3 and burst pacing to reveal hidden arrhythmogenic substrates. The execution of reliable in vivo electrophysiology requires: Precise Electrode Placement: Catheter electrodes must be positioned accurately within specific cardiac chambers (e.g., right ventricular apex, outflow tract) to ensure localized and reliable stimulation and recording of electrograms. Hemodynamic Monitoring: Continuous monitoring of blood pressure and heart rate is mandatory to ensure the physiological stability of the model during pacing and to interpret the hemodynamic impact of induced cardiac arrhythmias. Fractionated Electrogram Analysis: Recording high-resolution endocardial and epicardial electrograms allows for the identification of areas exhibiting "fractionation" (multiple, delayed, or fragmented deflections). These areas often represent anatomical or functional blocks that can initiate and maintain re-entrant cardiac arrhythmias. Autonomic Modulation: The inclusion of isoproterenol or other autonomic agonists/antagonists is often necessary to unmask latent or stress-induced cardiac arrhythmias, providing a more complete picture of the arrhythmogenic phenotype. The sheer volume and complexity of data generated by modern electrophysiological studies—whether from HT-APC, optical mapping, or in vivo recordings—mandate the use of sophisticated computational tools. Accurate analysis of these data sets is not merely post-processing; it is integral to deriving mechanistic conclusions about cardiac arrhythmias. Action Potential Duration (APD) Restitution Analysis: This is a crucial metric for predicting susceptibility to re-entry. It involves plotting APD as a function of the preceding diastolic interval (DI). A steep APD restitution curve (slope > 1) indicates increased instability and high risk of developing functional re-entrant cardiac arrhythmias. Power Spectrum Analysis (PSA): Used primarily in fibrillation studies, PSA involves applying a Fast Fourier Transform (FFT) to complex, disorganized electrograms. The dominant frequency (DF) derived from the spectrum provides a quantitative measure of the rate and organization of fibrillatory activity, differentiating between highly organized and highly disorganized cardiac arrhythmias. Computational Modeling and Simulation: Beyond simple analysis, biophysically detailed computer models of cardiac cells and tissues are employed to test hypotheses under controlled in silico conditions. These models integrate ion channel kinetics, gap junction function, and tissue structure to simulate the effects of specific genetic mutations or pharmacological interventions on the initiation and termination of cardiac arrhythmias. This predictive capacity is rapidly becoming essential for preclinical assessment. Activation Mapping and Isopotential Line Generation: Specialized software reconstructs the temporal sequence of electrical activation across the heart surface, producing isochronal maps. The spatial resolution of these maps is critical for pinpointing the origin of ectopic beats or defining the propagation characteristics of re-entry pathways responsible for cardiac arrhythmias. Electrophysiological tools and standardized protocols form the mechanistic cornerstone for understanding and mitigating the risk associated with cardiac arrhythmias. From the molecular precision of automated patch-clamp analysis to the spatiotemporal resolution of optical mapping and the integrated physiological insights from in vivo studies, a unified methodology is critical. The meticulous application of these techniques allows laboratory professionals to define precise genotype-phenotype correlations, identify novel antiarrhythmic targets, and validate therapeutic strategies. Continued advancement in data processing, particularly in computational modeling, is expected to accelerate the translation of basic science findings into clinical practice, ultimately improving the prognosis for patients affected by complex and life-threatening cardiac arrhythmias. What is the primary role of high-throughput patch-clamp in studying cardiac arrhythmias? The primary role is the rapid and quantitative measurement of ion channel function (kinetics, voltage dependence) in high-volume settings, which is essential for screening compounds and characterizing the functional defects caused by ion channel mutations associated with inherited cardiac arrhythmias. How does optical mapping enhance the understanding of complex cardiac arrhythmias? Optical mapping provides two-dimensional visualization of electrical wave propagation across intact cardiac tissue, allowing researchers to accurately identify the formation of re-entrant rotors and spiral waves that sustain ventricular and atrial cardiac arrhythmias, which cannot be achieved with point electrode recordings alone. What is the significance of the Action Potential Duration (APD) restitution curve in the context of cardiac arrhythmias? The APD restitution curve describes how the duration of the action potential changes based on the preceding diastolic interval. A steep restitution slope ( Which ion channel is often targeted pharmacologically to treat or prevent cardiac arrhythmias? The hERG channel (which mediates the 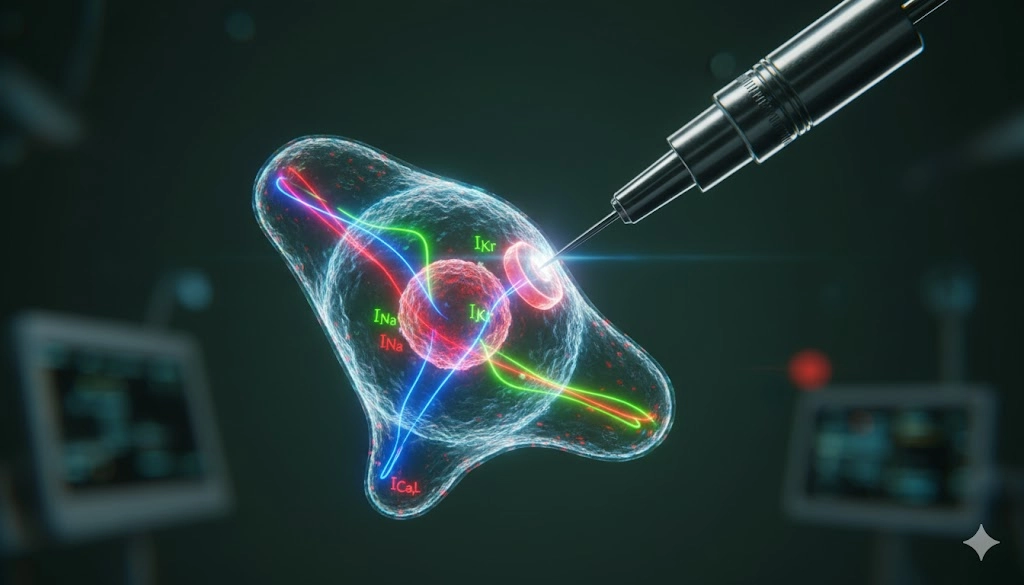
Advanced Tools for High-Throughput Ion Channel Profiling in Cardiac Arrhythmias
Protocols for Optical Mapping and Spatial Analysis of Arrhythmias
Key Preparations and Principles
Standardized In Vivo Pacing and Induction Protocols for Modeling Arrhythmias
Essential In Vivo Protocol Considerations
Data Analysis and Computational Modeling of Arrhythmia Dynamics
Key Computational Analysis Techniques
Advancing Translational Research and Therapeutic Strategies for Cardiac Arrhythmias
Frequently Asked Questions (FAQ)

Jan 09, 2026
Product News
BRANDTECH Scientific Introduces the Transferpette® pro Micropipette: A New Twist on Comfort and Control
The latest addition to its trusted line of precision liquid handling instruments, engineered for comfort, control, and repeatable accuracy.
Jan 06, 2026
Featured, Technical Insight
New Research Frontiers Unlocked by Next-Generation Flow Cytometry
Next-generation flow cytometry systems using acoustic focusing are opening entirely new areas of research that were previously impractical or inaccessible with conventional flow cytometers.

Jan 05, 2026
Buying Guides
The Bottom Line: How Smart Microcentrifuge Tube Choices Impact Lab Efficiency and Cost
Innovative microcentrifuge tube solutions are more than just lab consumables—they’re strategic tools that can reduce costs, improve outcomes, and support long-term sustainability goals.

Jan 05, 2026
Buying Guides
Future-Proofing Your Lab with Innovative Microcentrifuge Tube Solutions
As laboratories evolve to meet the growing demands of modern science, even the most basic tools—like microcentrifuge tubes—are being reimagined.

Jan 05, 2026
Buying Guides
Microcentrifuge Tube Innovations: Driving Sustainable Change
Integrating next-generation consumables into standard workflows can lead to a more sustainable and responsible research environment.

Jan 05, 2026
Buying Guides
Single Use Plastics: How to Manage these Major Contributors to Lab Waste
Reducing lab waste isn’t just a sustainability issue—it’s a financial and operational one, too.

Jan 05, 2026
Buying Guides
Common Microcentrifuge Tube Challenges in Sensitive Molecular Workflows
Key factors that can impact the performance of microcentrifuge tubes for PCR, qPCR, and NGS and other sensitive applications
Jan 05, 2026
Buying Guides
How to Research the Right Microcentrifuge Tubes for Your Application
Selecting the right microcentrifuge tubes starts with understanding the specific demands of your application.

Jan 05, 2026
Technical Insight
The Best Confocal Microscopes of 2026
Discover the best confocal microscopes of 2026 for advanced imaging. Compare top models from Zeiss, Evident, and Nikon for speed, resolution, and budget.

Dec 24, 2025
Featured, Popular Products, Technical Insight
Emerging Mass Spectrometry Technologies to Improve Intraoperative Diagnostics
Advances in mass spectrometry may soon reshape surgery, improving diagnostic accuracy and impacting post-operative outcomes